








Francesca Galiano
|
10/08/2022 - Last update 30/12/2022
D. Origo, A.G. Tarantino | Year 2018
Osteopathic manipulative treatment in pudendal neuralgia, a case report
Pathology:
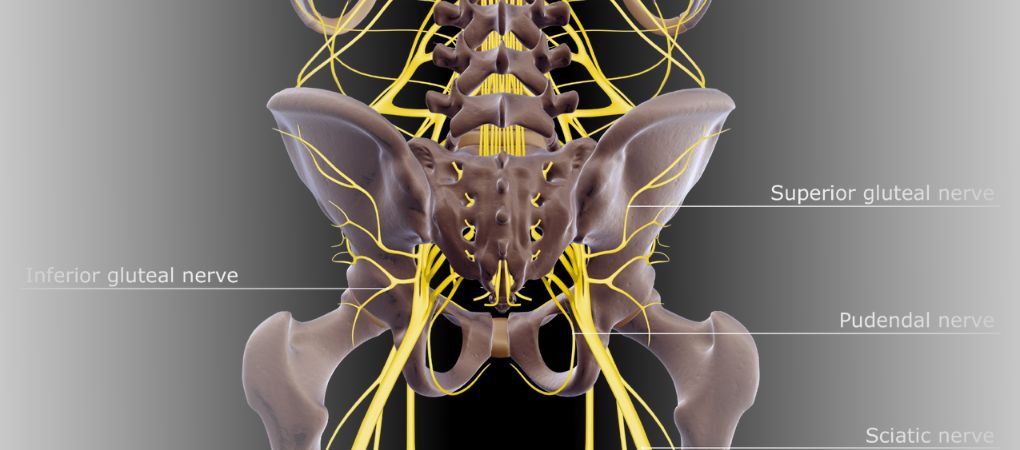
Neuralgia of the pudendal nerve
Type of study:
Case report
Date of publication of the study’:
2018/Feb/17
Purpose of the study
- Objective: to report the usefulness of OMT in treating a case of pudendal neuralgia
- Measured outcomes: intensity of pain through Visual Analogue Scale (VAS) and female National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI), disability through Oswestry Disability Index (ODI) and fear of movement through Tampa scale of kinesiophobia (TSK)
Participants
- Number: 1
- Description: a 40-year-old woman, with no previous pregnancies, working as a hospital employee, with intense and constant burning perineal pain, which radiated from the left side of the perineum to the genital area and was associated with vulvar pain, dyspareunia and perineal numbness. The pain would increase when she was seated. A pericoccygeal pain was also present. No pelvic organs’ dysfunctions were detected (eg, urinary incontinence), and the clinical history showed no gastrointestinal or gynecological inflammatory disease. However, a history of several past surgeries became apparent: one for pyloric stenosis and, because of a recurrent grade III hemorrhoids, subsequently evolved into anorectal fistula, two operations of hemorrhoidectomy and a lateral internal sphincterotomy, which left a retracted hypertrophic scar that was particularly painful in the left posterior quadrant. 2 weeks after this last surgery a pudendal neuralgia began and intensified over the following months. Consequently, after appropriate examinations, a diagnosis of pudendal nerve entrapment syndrome was issued by a neurologist.
A motor electroneurography revealed a smaller amplitude in the response of the left pudendal nerve, probably due to an entrapment inside the Alcock canal. In addition, the symptoms and pain met the Nantes criteria for pudendal neuralgia. The patient was then prescribed a 3-month pharmacological therapy. Since the doctor hypothesized a pelvic girdle dysfunction, they recommended osteopathic treatment in case of persistent symptoms.
The osteopathic structural evaluation showed tenderness in the muscles of the left buttock and pelvic floor, while palpation of the left sacrospinous, sacrotuberous, sacroiliac and lumbosacral ligaments on the left induced pain. The prone lumbar instability test and the straight-leg raise test were negative, while the Gillet tests on the left side and pain provocation test in the posterior pelvis were positive. Also the provocation test on the sacro-coccygeal joint came out positive.
Interventions and evaluations
- Evaluation of intensity of pain through VAS and NIH-CPSI, disability though ODI and fear of movement through TSK at baseline, after the pharmacological treatment, 1 and 6 months after OMT
- Pharmacological therapy: pregabalin, duloxetine and transdermal fentanyl for 3 months
5 weekly OMT over a month - OMT: direct and indirect fascial techniques based on the physical evaluation, paying particular attention to the double crush syndrome (pudendal canal and dura mater at the level of the sacral roots)
- in the first 2 sessions: pelvic floor release, balanced ligamentous tension of the sacroiliac joints, fascial unwinding of the hypogastric region, lumbosacral decompression, internal direct sacrococcygeal mobilization
- in the last 3 sessions: fascial unwinding of the thoracic diaphragm, the pelvic floor and the crural fascia, balanced ligamentous tensions of the sacrotuberous ligaments and of the extracranial fascia and dura mater both at the cranial base and at the sacrum
Results
Given her initial condition defined by high levels of pain and disability, a slight improvement in disability measured by ODI (48 to 29) and fear of movement assessed by TSK (51 to 41) emerged after 3 months of drug therapy. However, the pain remained more or less unchanged (VAS remained at 10 and NIH-CSPI went from 34 to 30). On the contrary, 1 month after the last session of OMT, improvements emerged in every aspect, particularly in pain (1.8 according to VAS and 7 according to NIH-CSPI). Furthermore, the disability value dropped further (from 29 to 9) and so did the fear of movement (from 41 to 20).
In addition, at this follow-up the function and provocation tests were negative. After 6 months, the scores of the various scales remained stable, thus showing lasting results over time.
Discussion
Unlike the pharmacological therapy carried on for 3 months, the OMT proved to have important positive repercussions on the health of the patient, significantly improving, in terms of pain and disability, the pudendal neuralgia. The result, accompanied by a total recovery of the ability to carry out daily activities, persisted for 6 months after the last OMT session.
Most likely, OMT showed a greater effect than pharmacological therapy because the multiple surgeries may have induced a number of fascial restrictions that induced a pro-inflammatory state only as a consequence. The fascial restrictions may then have favored greater nervous sensitivity, taking into account the likely presence of two conditions: pudendal neuralgia and double crush syndrome due to restrictions in the sacro-coccygeal region and at the level of the pelvic scar.
The review of Osteopedia
By Marco Chiera
Strengths: good and accurate description of the clinical case, thanks to the use of tables showing the timing of the study; follow-up at 1 and 6 months; interesting comparison between OMT and drug therapy, especially through the use of validated scales.
Limits: Like all case reports, it is not generalizable; a description of the study limits is missing.

Are you an osteopath?
Register and enjoy the membership benefits. Create your public profile and publish your studies. It's free!
Register now
School or training institution?
Register and enjoy the membership benefits. Create your public profile and publish your studies. It's free!
Register now
Do you want to become an osteopath? Are you a student?
Register and enjoy the membership benefits. Create your public profile and publish your studies. It's free!
Register now